| Stiffness of the fingers is a common problem following either closed or open injury. The moving parts of fingers are often glued together by scar tissue following injury, and if movement can not be recovered through therapy and time, and if all other conditions are favorable (wound maturation, patient motivation, available therapy, absence of infection or mechanical impediment, etc. ), tenolysis may be helpful. A practical guideline is that the expected final active range of motion will be halfway between the preoperative active and passive ranges of motion. These cases illustrate extensor tenolysis at the proximal and distal interphalangeal joints after open injury. |
| Click on each image for a larger picture |
| Case 1:
This gentleman sustained a laceration of the dorsal finger at the level of the proximal interphalangeal joint. The treating surgeon repaired the extensor tendon. After extensive therapy, his finger was still quite stiff: |
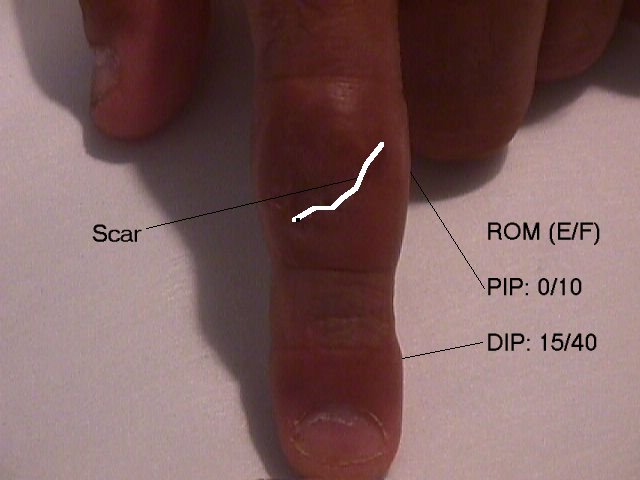 |
| Posture of the finger with attempted flexion: minimal movement of the proximal interphalangeal joint, extensor lag of the distal interphalangeal joint, similar to a stiff swan neck deformity: |
 |
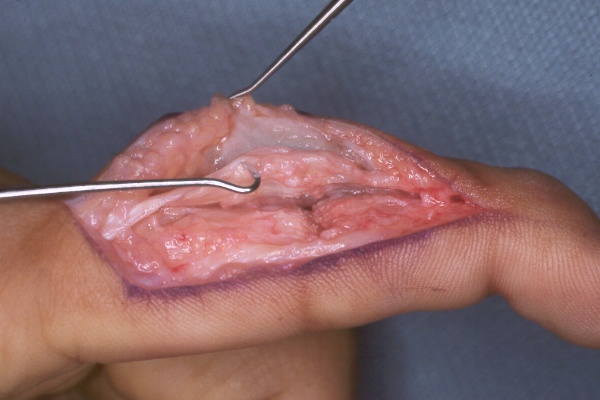
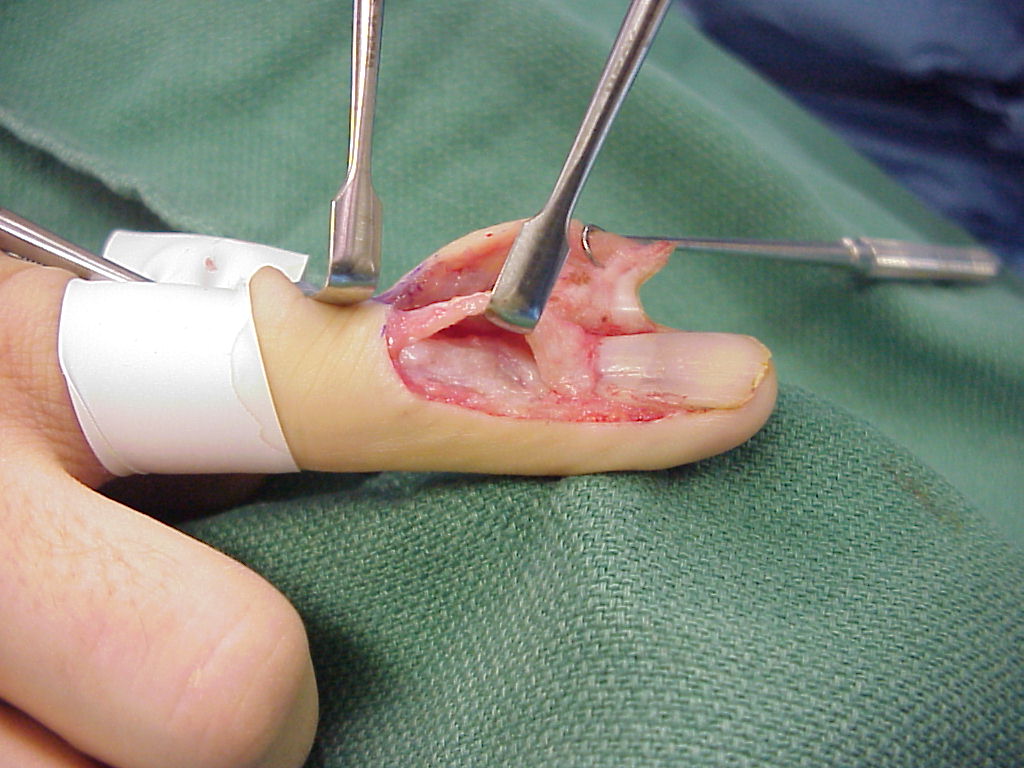
| At surgery, the patient was found to have dense extensor tendon adhesions. The nonabsorbable sutures used for repair were removed. A Fowler swan neck type release was performed, releasing the central slip attachment to the base of the middle phalanx, removing the dorsal joint capsule and releasing both collateral ligaments: |
 |
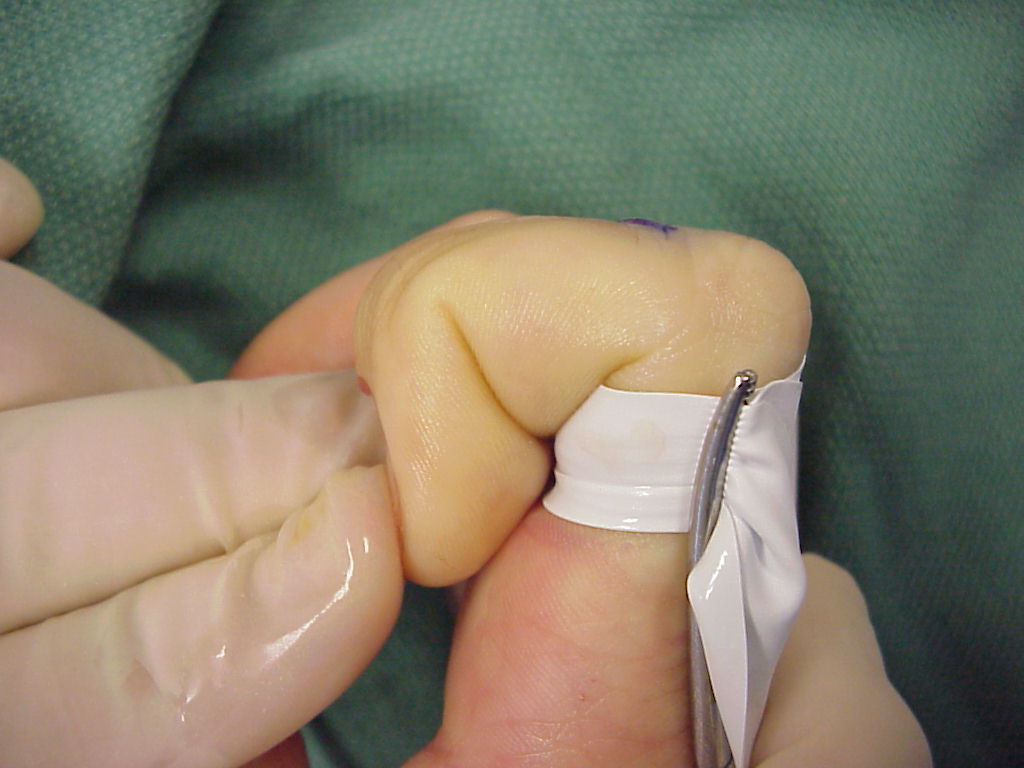
| This allowed improved range of motion in the operating room: |
 |
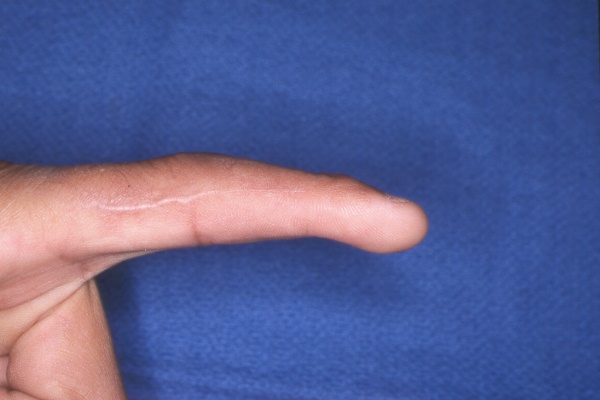
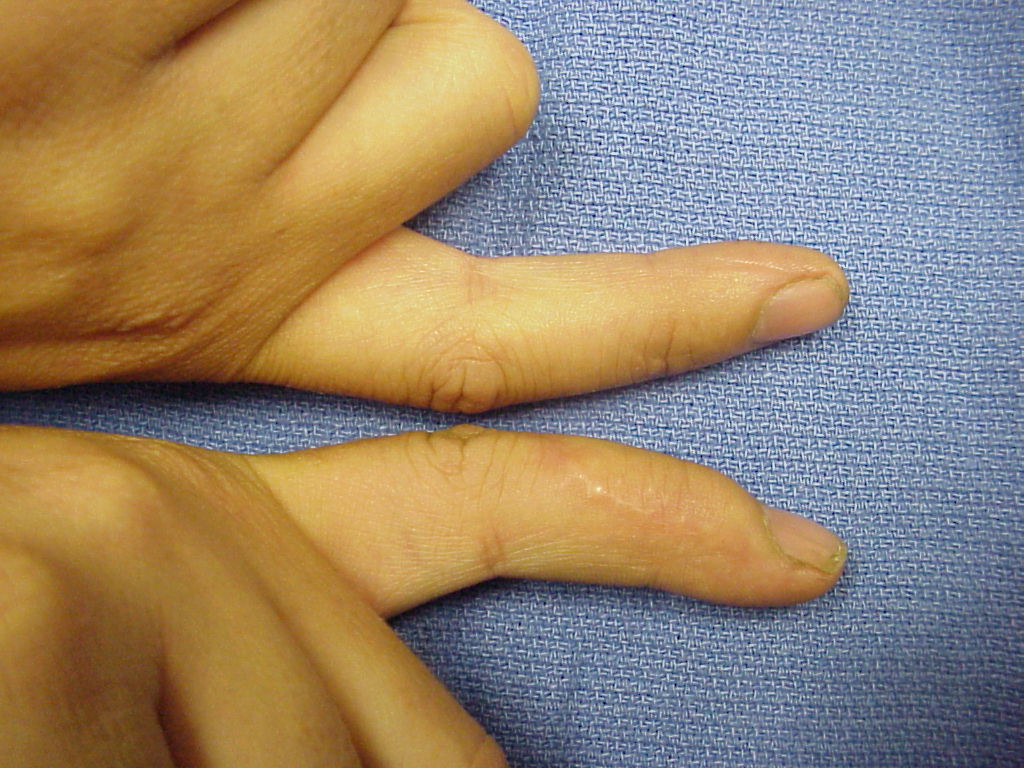
| Several months later, the patient had
improved (although not normal) range of motion.
Extension: |
 |
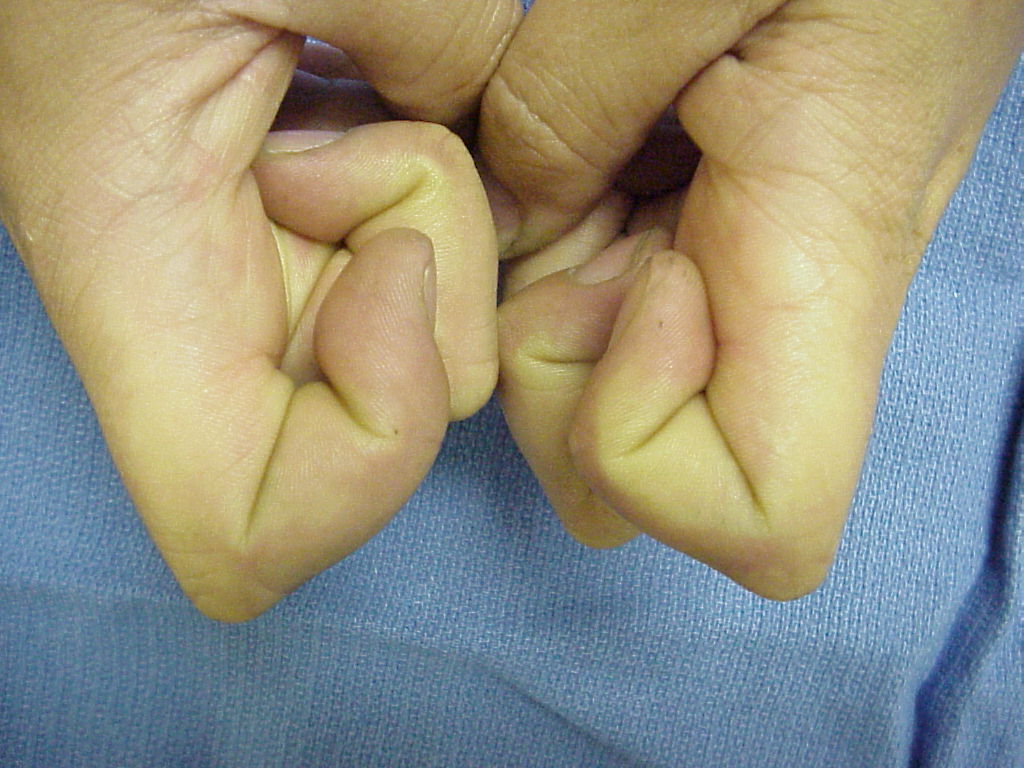
| Flexion: |
 |
| Another option for tenolysis access is through a proximal window, sliding a Freer and then a Beaver #9081 arthro-loc end cutting blade from an entry point proximal to the sagittal bands. From this point, one can free a plane over the entire proximal phalanx out to the central slip. Because the dorsal lip of the base of the middle phalanx sits a bit dorsal to the proximal phalanx head, the blade usually follows the proximal phalanx dorsum, disinserts the proximal joint capsule attachments and then stops as it abuts the base of the middle phalanx. |
 |
| Case 2:
This gentleman sustained a crush avulsion of the dorsal aspect of the distal interphalangeal joint. He took this picture with a digital camera a few days after injury: |
 |
| Months later, he sought evaluation because he had neither active nor passive range of motion of his distal interphalangeal joint: |
 |
| At surgery, the extensor tendon was released from the bone and skin, the dorsal joint capsule was excised, and collateral ligaments were released: |
 |
| Range of motion in the operating room: |
 |
 |
| Final active range of motion: |
 |
 |
| Search for...
extensor tenolysis tenoarthrolysis |
Case Examples Index Page | e-Hand Home |