| Chronic
scapholunate ligament instability
remains an unsolved problem. A variety of approaches have been
described,
including bone procedures, such as limited intercarpal fusions and
proximal
row carpectomy, as well as soft tissue procedures of ligament
reconstruction
such as direct repair, capsulodesis, tendon graft, and
bone-ligament-bone
graft. None are entirely satisfactory because of the common outcome of
late failure. These cases demonstrate an unpublished soft tissue
technique,
employing a strip of extensor retinaculum attached to the dorsal
triquetrum,
inserted into the distal dorsal scaphoid to construct a dorsal
intercarpal
support along the path of the normal scaphotriquetral ligament. In
theory,
this recreates a physiologic force vector preventing excessive palmar
flexion
of the scaphoid. In a small series, results are comparable to other
soft
tissue - that is, patients had pain relief, but some loss of motion,
and
gradual recurrence of the scapholunate gap during the first
postoperative
year.
These cases are presented simply to show some details of the technique. The indications and outcome for this approach remain to be established. |
| Click on each image for a larger picture |
| The scaphoid, lunate and triquetrum form a somewhat flexible unit having the shape of the arc of a spiral and interesting biomechanics. For example, when the wrist moves from radial to ulnar deviation, the proximal carpal bones move in a perpendicular direction, rotating from palmar to dorsal flexion. Here, the three proximal carpal bones are illustrated as one unit: |
 |
| This pattern of motion is demonstrated here with Lego figures. Neutral wrist position: |
 |
| Radial deviation: The scaphoid palmar flexes to accomodate the descent of the radial wrist. |
 |
| Ulnar deviation: The proximal row dorsiflexes, bringing the scaphoid up and the triquetrum down to accomodate the proximal movement of the ulnar wrist in ulnar deviation. |
 |
| Scapholunate dissociation: The scaphoid palmar flexes and translates away from the lunate-triquetrum complex, which dorsiflexes. |
 |
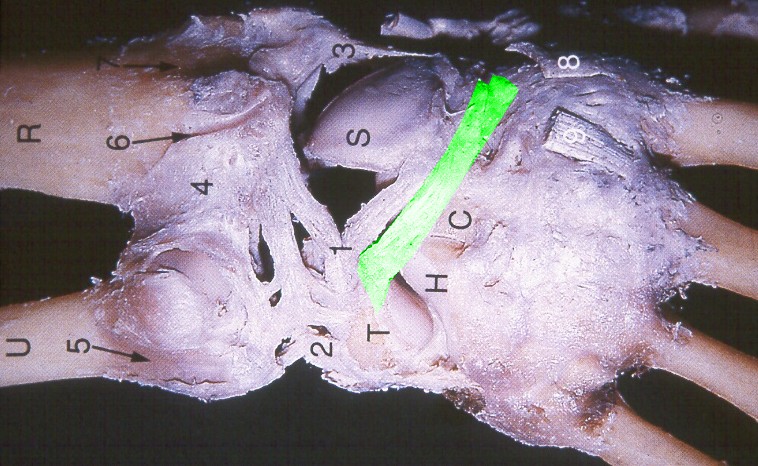
| Here's the idea behind this procedure: Normal course of the dorsal triquetroscaphoid ligament (image modified from Zancolli E A, Cozzi E P 1992 Atlas of Surgical Anatomy of the Hand. Churchill Livingstone, Edinburgh.) |
 |
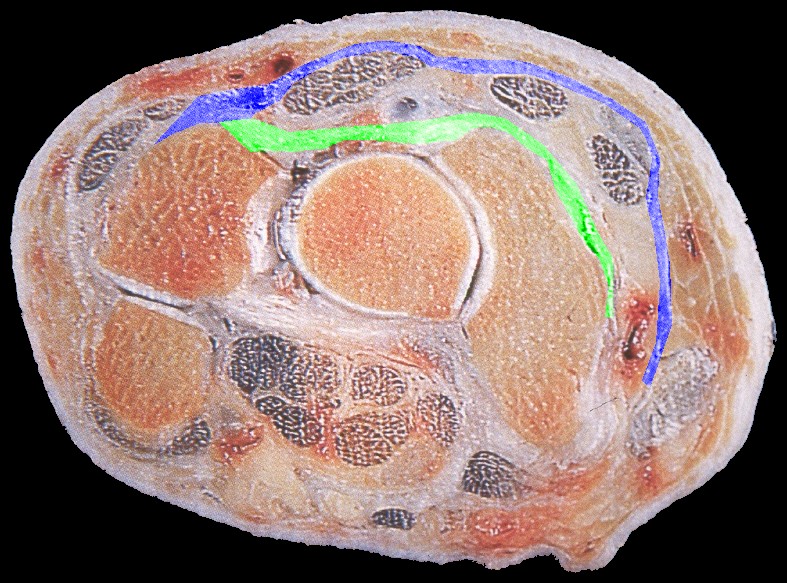
| Normal relationship of the dorsal intercarpal ligaments (green) and extensor retinaculum (blue) at the level of the triquetrum. (image modified from Zancolli E A, Cozzi E P 1992 Atlas of Surgical Anatomy of the Hand. Churchill Livingstone, Edinburgh.) |
 |
| Case 1. Chronic complete scapholunate ligament disruption seen on MRI |
 |
| Palmar flexion of the scaphoid, lunate dorsiflexion. |
 |
| Scapholunate diastasis. |
 |
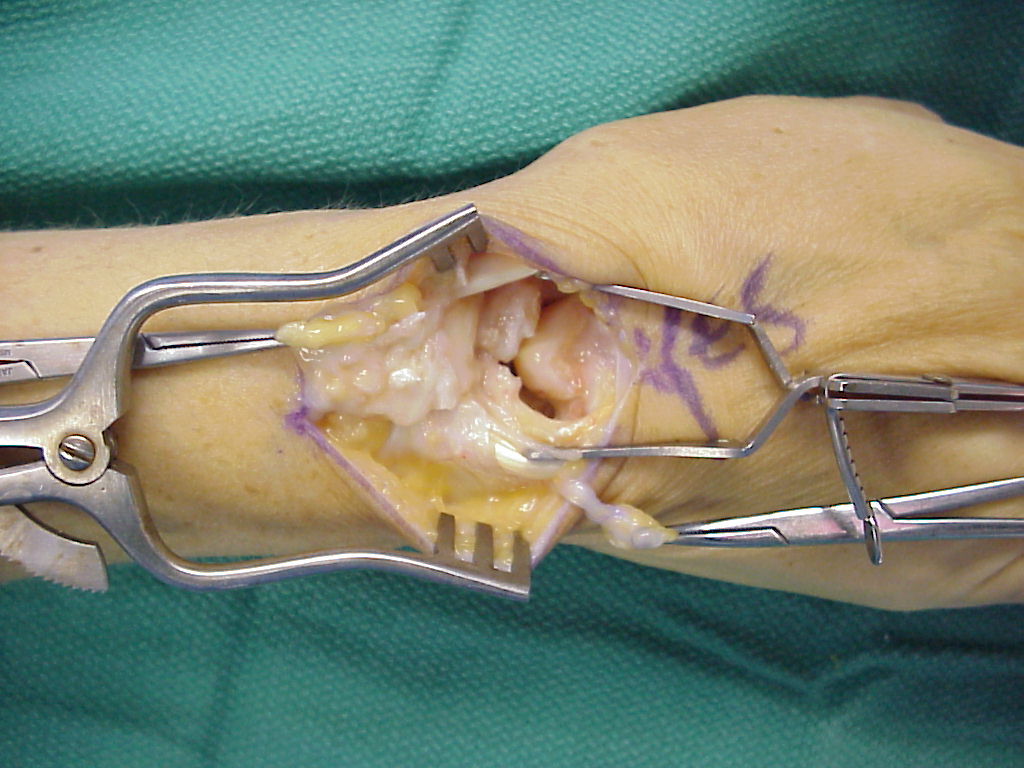
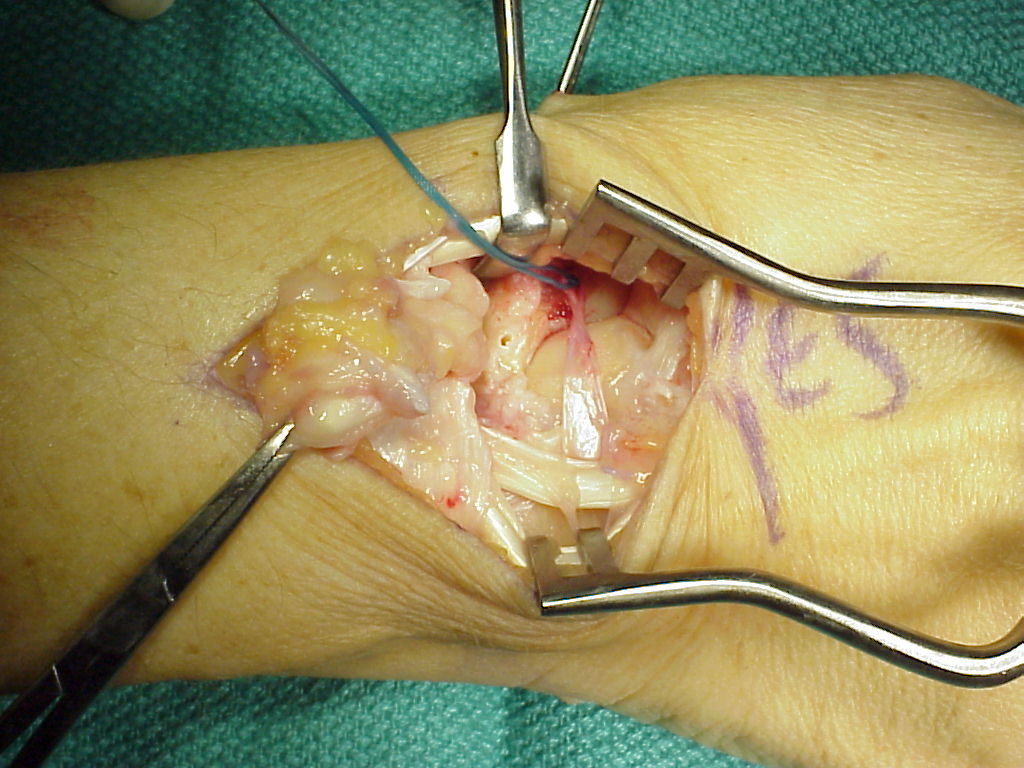
| Complete scapholunate ligament disruption seen intraoperatively. A strip of extensor retinaculum is harvested as a ligament graft, left attached to the triquetrum. (Right hand, fingers to the right) |
 |
| Intraoperative correction of scapholunate rotation using K-wires as joysticks on each bone. |
 |
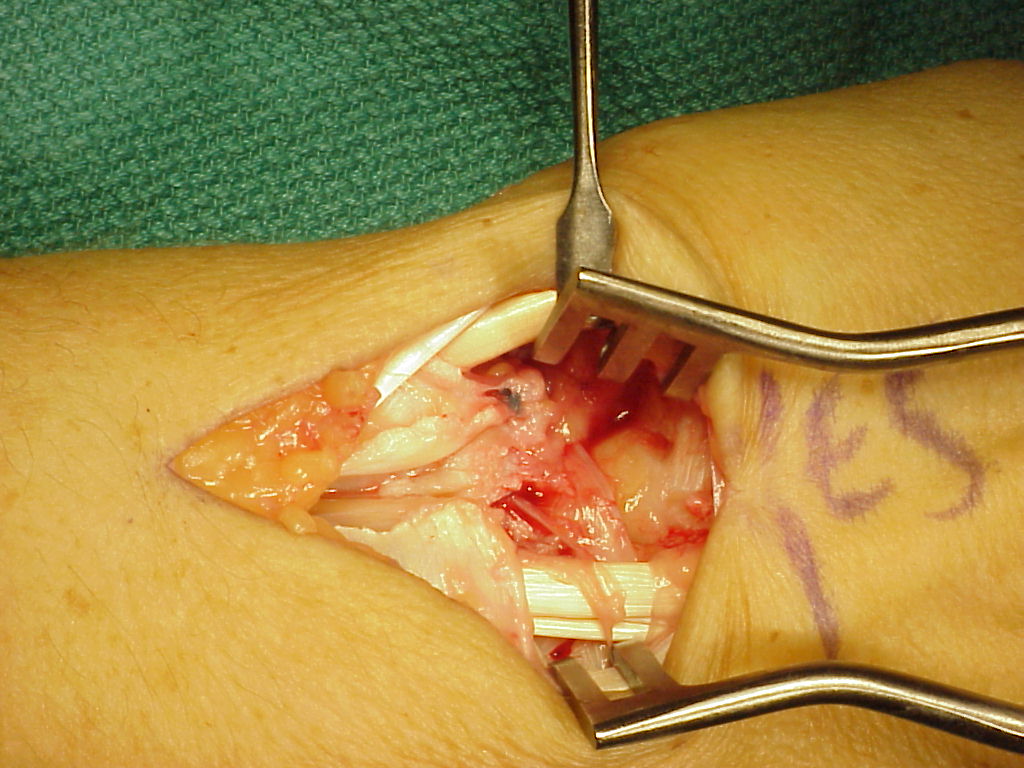
| The retinaculum graft crosses over the capitate and is secured to a trough created in the dorsal distal scaphoid using a bone anchor. |
 |
| In this case, a dorsal capsulodesis was also secured to the same anchor attachment. Additionally, the original ligament remnant was unfurled from the lunate and reattached to the proximal scaphoid using a second bone anchor - a 3 point reconstruction. |
 |
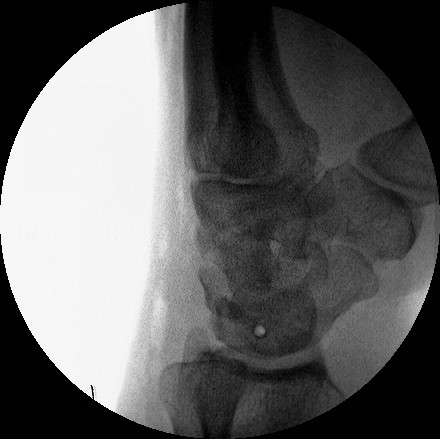
| Scapholunate pins and bone anchors - intraoperative fluoroscopy. |
 |
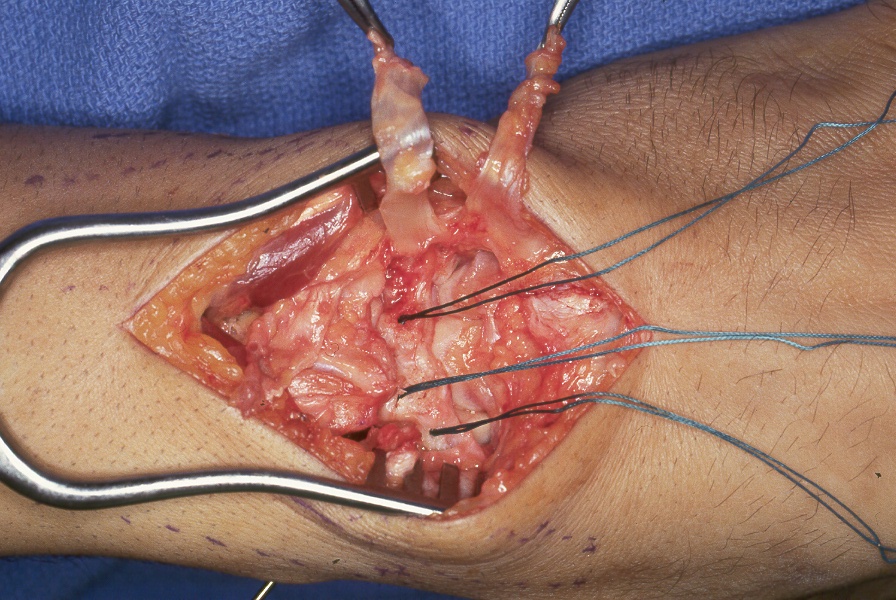
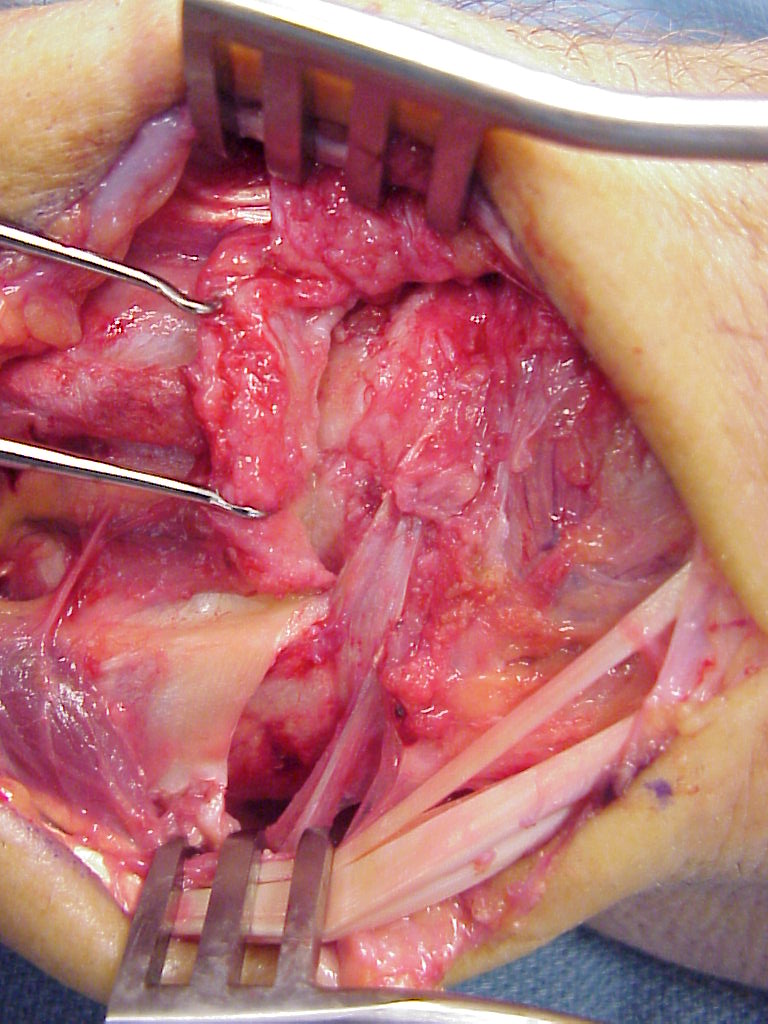
| Case 2. Direct repair of scapholunate ligament and retinaculum transfer (Ragnell retractor beneath). (Right hand, fingers to the right) |
 |
| Closure of retinaculum showing the area of the donor strip. |
 |
| Preop |
 |
| Postop. |
 |
| Case 3. Two strips were used, one to the distal scaphoid and one for a direct scapholunate segment. (Left hand, fingers to the right) |
 |
 |
| Case 4. Preop dynamic instability |
 |
| In this case, the scapholunate repair was stabilized with absorbable (Bionx) screws. Provisional fixation for two screws with a pin and a drill. |
 |
| These were then replaced with screws, which are radiolucent. |
 |
| Lucency where a screw lies. |
 |
| Retinaculum transfer. The screws were cut flush with the bone, ends barely visible here in the scaphoid and lunate. (Right hand, fingers to the right) |
 |
| Unfortunately, the screws did not provide adequate stability and lost purchase about six weeks postoperatively. Symptoms remained improved despite early radiographic recurrence of scapholunate diastasis. |
| Search for...
scapholunate ligament injury wrist capsulodesis |
Case Examples Index Page | e-Hand home |